
Pain in People with Intellectual Disabilities
The Loeser model (Loeser, 1980) illustrates what differs in the experience of pain for people with intellectual disabilities.
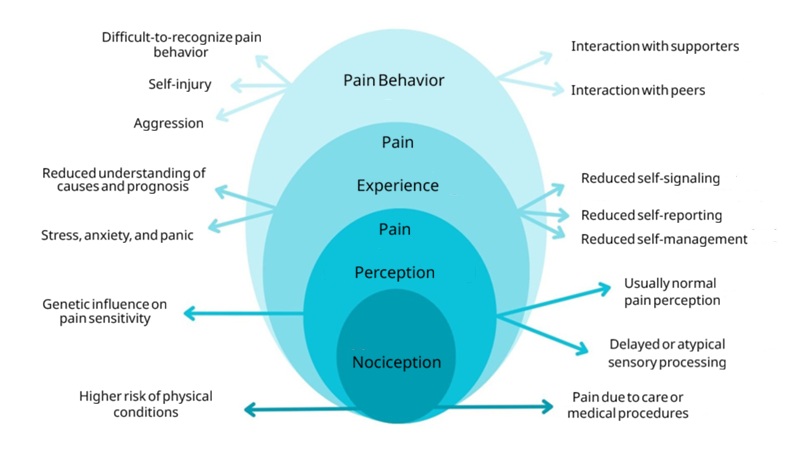
Loeser's model supplemented with challenges specific to people with intellectual disabilities (source: Guideline on Pain in People with Intellectual Disabilities, SKILZ, 2025)
People with intellectual disabilities have an increased risk of painful conditions, such as injuries, musculoskeletal disorders (e.g., spasticity), and gastrointestinal diseases (e.g., reflux). Additionally, impaired functioning of the central nervous system (in genetic syndromes or congenital central nervous system disorders) and insufficient inhibition of anxiety due to limited understanding can lead to sensitization (increased sensitivity of pain sensors) and heightened pain perception.
For pain recognition, people with intellectual disabilities often depend on caregivers. Due to the wide variety of pain expressions and difficulty recognizing pain behavior, pain detection by caregivers is complex. People with intellectual disabilities also have limited self-management abilities, making caregiver support essential. Both non-pharmacological and pharmacological pain treatment are complicated by the intellectual disability. Factors such as limitations in comprehension—and thus motivation and ability to follow instructions—comorbidities (other conditions or diseases), and polypharmacy (use of multiple medications) play a role. Evaluating treatment is also complex because self-reporting often cannot be used as an evaluation criterion. The above factors increase the risk of underrecognition, underdiagnosis, and undertreatment of pain.
Further background information on pain in people with intellectual disabilities can be found in this publication (p. 14 – Pain Challenge Inventory, NTPP).
Sensory processing issues and problem behavior are common in people with intellectual disabilities. These issues can be related to pain:
- Sensory processing and pain
- Changes in sensory information processing frequently occur in people with intellectual disabilities, particularly in those who also have autism spectrum disorder. These changes, combined with limited coping strategies, can lead to discomfort and difficult-to-understand behavior. Research on the relationship between sensory processing and pain shows that similar neurophysiological processes are involved in pain and sensory overresponsivity (hypersensitivity to one or more senses). For more information, see: Sensory Modulation Disorder (SMD) and Pain: A New Perspective – PubMed. It may be worthwhile to further investigate whether regulatory strategies from sensory processing could also influence (chronic) pain.
- Problem behavior and pain
- Loeser's model clarifies that a pain experience can result in pain behavior. For people with intellectual disabilities, behavior is sometimes the only way to communicate pain. Through interaction with the client system, behavior can be reinforced, potentially leading to problem behavior (aggression, self-injury). As pain and the interaction persist, the relationship becomes increasingly complex, and more factors come into play. In cases of problem behavior and self-injury, pain is rarely the sole influencing factor. For more information on this topic, see the Center for Consultation and Expertise (CCE) and the Problem Behavior Guideline by the Dutch Association of Physicians for Intellectual Disabilities (NVAVG) (currently under revision by SKILZ).